


Life After Regions
Exploring Continuous Distribution Systems Health disparities continue to be a challenge that we, as a community, must address for the well being and future of our patients. In the field of transplantation, there are vast geographic disparities. Prior to the continuous distribution mandate, in liver transplantation alone, 7 out of 11 regions had a relative rate of transplantation that differed significantly from the nation, a clear sign that change was in order. To aid the closing of this health gap, the OPTN Board of Directors endorsed the development of continuous distribution systems in December 2018.
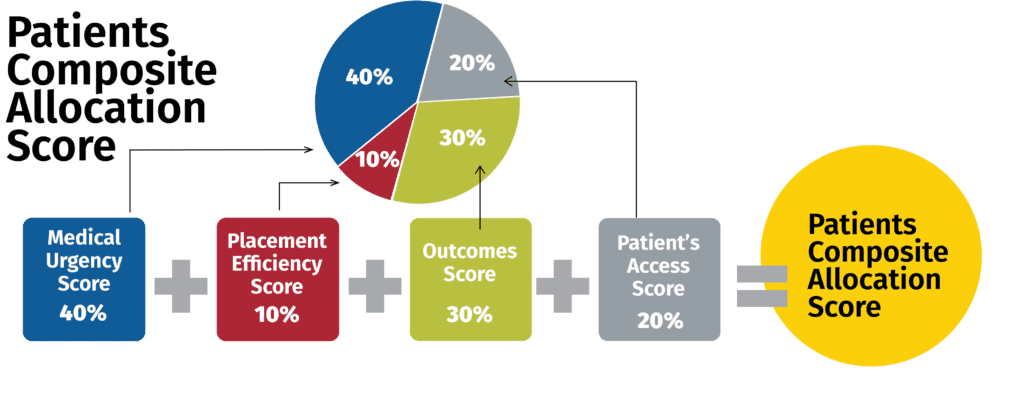
What is Continuous Distribution?
Continuous distribution utilizes a statistical formula that combines the following key clinical factors:
- Medical urgency
- Placement efficiency
- Outcomes score
- Candidate access score
The formula then creates a relative distribution score. The relative distribution score is considered without any absolute geographic boundary so that candidates who have the best combinations of factors receive priority.
While this is an ongoing process, there are some updates that have already been made to the distribution systems for heart, lung, liver, kidney, pancreas, and Vascularized Composite Allografts (VCAs). In the future, we can expect to see further updates regarding next steps for lowering disparities within our patient populations. The current features and effects of these changes include:
Heart Allocation System
- Continuous distribution became effective Jan. 9, 2019 using 250 nm
- Six new medical urgency statuses (Click here for more information)
- Hearts can be distributed up to 500 miles + DSA for the new Statuses 1 & 2
- Expected effect: reduce waiting list deaths
Liver Allocation System
- New policy implemented in Feb. 2020, now using 500nm – removes DSAs and Regions from liver distribution
- National Liver Review Board – implemented April 2019
- Enhanced Liver Distribution/Acuity Circle Liver Distribution & Allocation – implemented February 2020
- Distribution concepts are in the process of being modeled to utilize fixed distance circles around the donor hospital ▷ Expected effect: More transplants for the sickest candidates and broader
Lung Allocation System
- Designated Service Areas (DSAs) were removed in 2017, now using 500nm
- Ongoing monitoring and discussions continue within UNOS Research (6 Month Report of DSA Removal) and the Thoracic Committee ▷ Expected effect: More transplants for the sickest candidates
Kidney & Pancreas Allocation System
- Implementation of Kidney and Pancreas circles by December 2020
- Replace DSA and Region with a fixed distance circle with a radius of 250 nm
- Add proximity points to a candidate’s total allocation score based on the distance of candidate’s center from the donor hospital ▷ Expected effect: More transplants for the sickest candidates
The content of this issue is based on a webinar presentation by David C. Mulligan, MD, FACS, FAASLD, FAST, Yale University/Yale New Haven Health System. A special thanks to Dr. Mulligan for his contributions to this in-service.


