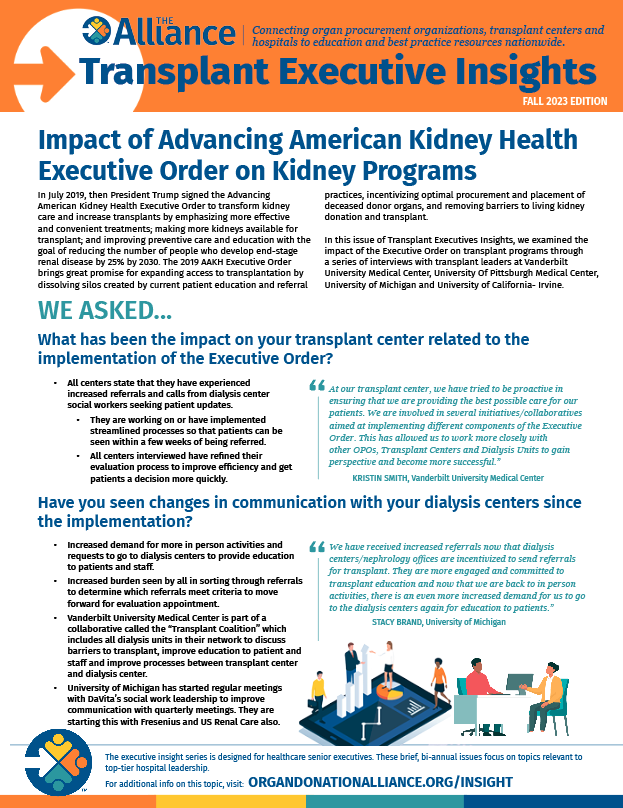
In July 2019, then President Trump signed the Advancing American Kidney Health Executive Order to transform kidney care and increase transplants by emphasizing more effective and convenient treatments; making more kidneys available for transplant; and improving preventive care and education with the goal of reducing the number of people who develop end-stage renal disease by 25% by 2030. The 2019 AAKH Executive Order brings great promise for expanding access to transplantation by dissolving silos created by current patient education and referral practices, incentivizing optimal procurement and placement of deceased donor organs, and removing barriers to living kidney donation and transplant.
In this issue of Transplant Executives Insights, we examined the impact of the Executive Order on transplant programs through a series of interviews with transplant leaders at Vanderbilt University Medical Center, University Of Pittsburgh Medical Center, University of Michigan and University of California- Irvine.
We asked…
What has been the impact on your transplant center related to the implementation of the Executive Order?
- All centers state that they have experienced increased referrals and calls from dialysis center social workers seeking patient updates.
- They are working on or have implemented streamlined processes so that patients can be seen within a few weeks of being referred.
- All centers interviewed have refined their evaluation process to improve efficiency and get patients a decision more quickly.
At our transplant center, we have tried to be proactive in ensuring that we are providing the best possible care for our patients. We are involved in several initiatives/collaboratives aimed at implementing different components of the Executive Order. This has allowed us to work more closely with other OPOs, Transplant Centers and Dialysis Units to gain perspective and become more successful. — Vanderbilt University Medical Center
Have you observed changes in communication with your dialysis centers since the implementation?
- Increased demand for more in person activities and requests to go to dialysis centers to provide education to patients and staff.
- Increased burden seen by all in sorting through referrals to determine which referrals meet criteria to move forward for evaluation appointment.
- Vanderbilt University Medical Center is part of a collaborative called the “Transplant Coalition” which includes all dialysis units in their network to discuss barriers to transplant, improve education to patient and staff and improve processes between transplant center and dialysis center.
- University of Michigan has started regular meetings with DaVita’s social work leadership to improve communication with quarterly meetings. They are starting this with Fresenius and US Renal Care also.
We have received increased referrals now that dialysis centers/nephrology offices are incentivized to send referrals for transplant. They are more engaged and committed to transplant education and now that we are back to in person activities, there is an even more increased demand for us to go to the dialysis centers again for education to patients. — Stacy Brand, University of Michigan
What strategies or initiatives have you evaluated or implemented in dealing with the impact of the Executive Order?
- Staffing
- Focus on outreach and continuing to expand based on what is happening with our partners
- Two centers have dedicated outreach nurses /liaison that has helped stay in front of additional demand
- One center added a Dialysis Unit Liaison to their pre-transplant team
- Another center added a 2nd living donor coordinator
- IT/Software solutions
- One center created an electronic, automated monthly report that is sent from EMR to all referring providers and dialysis units that contains a list of referred patients and their current phase within the transplant process
- Some centers are reviewing software options such as Care Dx, TRex and TXAccess. Found drawbacks with integration of some 3rd party software into current hospital EMR systems
- Another drawback to software solutions is the burden of the cost and the resources and bandwidth to teach and train dialysis unit staff on it. With high turnover in dialysis units, this could prove difficult and time consuming
- Education
- Created education documents for dialysis units and patients on the transplant process, including the referral process, to help break down barriers
- Provide ongoing education to staff to provide context and encourage a shared vision among the team
- Outreach roles provide education to dialysis center social workers, managed care groups, nephrologists
- Additionally, one transplant center hosts a large symposium yearly, open to community nephrologists and dialysis centers
- Other outreach efforts
- Involved in collaboratives such as End Stage Renal Disease Treatment Choices Learning Collaborative (ETCLC). This has provided an additional layer of perspective on what other OPOs and Transplant Centers are doing to meet the goals of the executive order
- Liaison with managed care groups
- Education offerings to public on living donation options
How do you deal with turned down referrals?
- Work to include when/if a patient is eligible for re-referral and what criteria must be met in communication with the dialysis center and referring MD.
- As part of the selection process, we make an effort to clearly document if/when a patient is eligible for re-referral and what criteria must be met. This information is shared with the patient, referring provider and dialysis unit. Although the patient may be re-referred outside of these parameters, we are able to easily see from our documentation if the referral is appropriate and can make the decision from there. The extra work on the front end saves a tremendous amount of time later
What level of transparency do you have with selection criteria for not accepting referral?
- Openly share selection criteria.
- Provided main selection criteria to dialysis units and referring providers as part of the education by the Dialysis Unit Liaison.
- Frequent updates to criteria as situations arise to ensure it remains accurate and up to date.
We are doing a pre-screen of referrals prior to starting a full evaluation. If the patient clearly does not meet our criteria. Low Cardiac Ejection Fraction; COPD and still smoking etc. We tell them over the phone they are not a candidate and send them a letter. This avoids us using a full evaluation appt. — Kim Barnett, University Of Pittsburgh Medical Center
How are you turning potentially negative interactions into education opportunities?
- Negative interactions tend to spur conversations that result in policy changes or development of educational materials to prevent those same interactions in the future.
- With increased referrals that do not progress to listings and backlogs that are occurring, the outreach coordinator uses this opportunity to re-educate on selection criteria and be available to collaborate and partner with all the dialysis centers and community nephrologists.
- The goal is to facilitate transplant as a treatment option for appropriate recipients, it’s not always easy, but we work to maintain good relationships with our dialysis units by being transparent and providing as much education as possible.
Any additional comments or thoughts that you would like to share?/strong>
- Meeting with the dialysis centers and referring physicians gives us the opportunity to explain the “why” behind many of our decisions that they may not understand.
- Having the dedicated outreach role already in place has been very helpful because the trusted relationship was in place.
The transplant center does not have a data metric they follow in relation to the outreach role, but the feedback from dialysis centers regarding the outreach role is very positive. They appreciate having a reliable contact that can handle all aspects of the referral process and can be reached at all times. — Heather Abrari, University of California-Irvine