Normothermic regional perfusion (NRP) is an in-situ perfusion of a portion of the donor’s body with the aid of mechanical organ support. This practice is utilized in a growing number of donation after circulatory determination of death (DCD) cases.
The overall advantage of NRP is that organs previously not utilized can now be utilized for transplantation, allowing for improved stewardship of the gift from the donor and their family and providing hope for those in need of a life-saving transplant.
As with many new approaches or procedures in medicine, NRP comes with legal and ethical considerations, clinical considerations, as well as operational considerations. This issue will focus on the clinical aspects of NRP.
There are two approaches to NRP:
- Thoracic-abdominal (TA)-NRP – in which the thoracic and abdominal organs are perfused. This approach is utilized for DCD heart recovery.
- Abdominal (A)-NRP – in which only the abdominal organs are perfused.
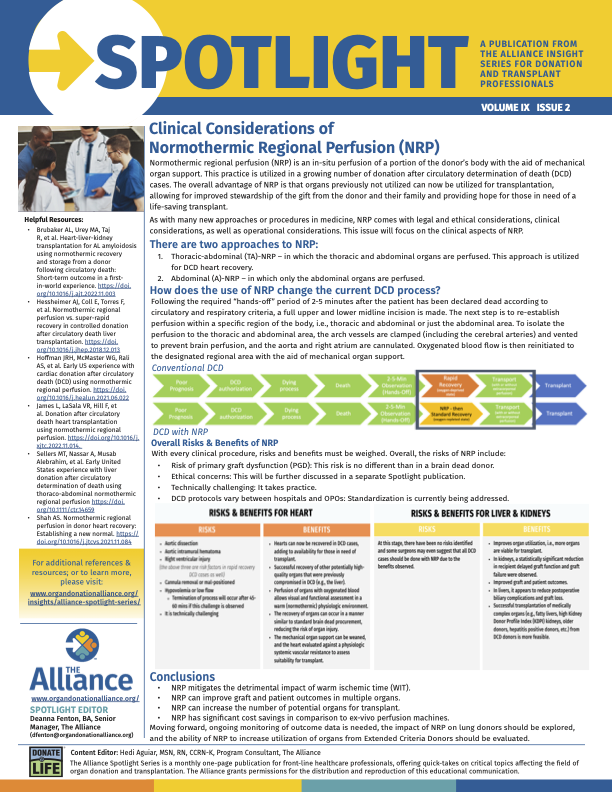
How does the use of NRP change the current DCD process?
Following the required “hands-off” period of 2-5 minutes after the patient has been declared dead according to circulatory and respiratory criteria, a full upper and lower midline incision is made. The next step is to re-establish perfusion within a specific region of the body, i.e., thoracic and abdominal or just the abdominal area. To isolate the perfusion to the thoracic and abdominal area, the arch vessels are clamped (including the cerebral arteries) and vented to prevent brain perfusion, and the aorta and right atrium are cannulated. Oxygenated blood flow is then reinitiated to the designated regional area with the aid of mechanical organ support.

Risks & Benefits of NRP
With every clinical procedure, risks and benefits must be weighed.
Overall, the Risks of NRP are:
- Risk of primary graft dysfunction (PGD): This risk is no different than in a brain dead donor.
- Ethical concerns: This will be further discussed in a separate Spotlight publication.
- Technically challenging: It takes practice.
- DCD protocols vary between hospitals and OPOs: Standardization is currently being addressed.
TA-NRP Risks & Benefits:
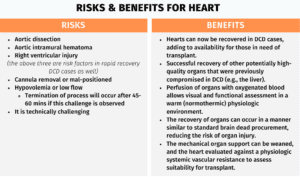
**It is worth noting that even if the above complications occur, the abdominal organs are still being perfused and can be recovered for transplant.
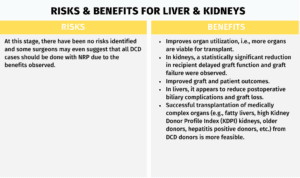
A-NRP Risks & Benefits:
Conclusion:
- NRP mitigates the detrimental impact of warm ischemic time (WIT).
- NRP can improve graft and patient outcomes in multiple organs.
- NRP can increase the number of potential organs for transplant.
- NRP has significant cost savings in comparison to ex-vivo perfusion machines.
Moving forward, ongoing monitoring of outcome data is needed, the impact of NRP on lung donors should be explored, and the ability of NRP to increase utilization of organs from Extended Criteria Donors should be evaluated.